
Advantages of statins might have been exaggerated
Cholesterol-bringing down statins are one of the world's most usually utilized medications. They were first endorsed for individuals with a high gamble of cardiovascular sickness in 1987. By 2020, worldwide deals were assessed to have moved toward US$1 trillion (£764 billion).
Notwithstanding, there has been a continuous discussion about regardless of whether statins are over-recommended. Does each and every individual who takes them truly benefit from them? To find out, my partners and I found 21 significant clinical preliminaries and investigated the consolidated information (north of 140,000 members) in what the future held meta-examination.
We posed two inquiries: is it best to bring down LDL cholesterol (once in a while known as "terrible" cholesterol) however much as could reasonably be expected to lessen the gamble of cardiovascular failure, stroke or unexpected passing? Also, how do the advantages of statins contrast when it accompanies diminishing the gamble of these occasions?
In reply to the main inquiry, we observed a shockingly feeble and conflicting connection between the level of decrease in LDL cholesterol from taking statins and an individual's risk of having a coronary episode or stroke, or kicking the bucket during the time for testing. In certain preliminaries, decreases in LDL cholesterol were related with huge decreases in the gamble of kicking the bucket, however in others, decreases in LDL cholesterol didn't diminish this gamble.
This is a significant finding on the grounds that clinical rules have extended the extent of individuals qualified for statins as "great" LDL cholesterol levels were steadily brought down. For instance, one review assessed a 600% increment in qualification for statins somewhere in the range of 1987 and 2016.
The extent of individuals in Europe
qualified for statins
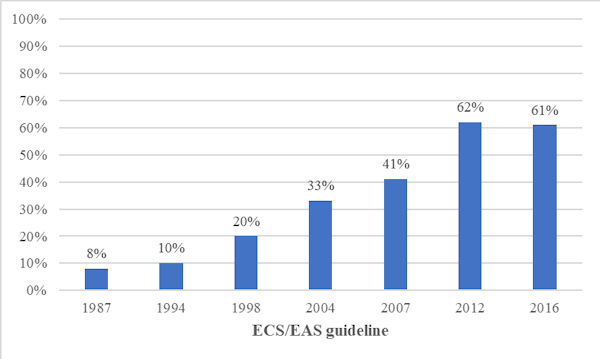
Proportion of people eligible for statins,
according to the European Society of Cardiology (ESC) and the European Atherosclerosis
Society (EAS). British Journal of General Practice, 69(683),
pp.e373-e380
As to second question, we saw two sorts of hazard decrease: relative gamble decrease and outright gamble decrease. Envision your possibility kicking the bucket from a specific condition rashly is 0.2%, and there's a medication that diminishes your possibility passing on to 0.1%. In relative terms (relative gamble decrease), your possibility passing on has been split, or diminished by half. However, in outright terms (outright gamble decrease), your possibility biting the dust has just gone somewhere around 0.1%.
In spite of the fact that there is a half relative gamble decrease, is it a significant contrast? Could it be advantageous to change to this medication, especially assuming there are aftereffects related with it? Outright gamble decrease presents a more clear picture and makes it simpler for individuals to settle on informed choices.
In our review, distributed in Jama Internal Medicine, we observed that the outright gamble decrease from taking statins was unassuming contrasted and the general gamble decrease. The general gamble decrease for those taking statins contrasted and the individuals who didn't was 9% for passings, 29% for cardiovascular failures and 14% for strokes. However the outright gamble decrease of kicking the bucket, having a coronary failure or stroke was 0.8%, 1.3% and 0.4% individually.
Outright gamble decrease contrasted and relative gamble decrease

Absolute risk reduction compared with relative
risk reduction. Jama Internal Medicine
Individual contrasts
A further thought is that preliminaries report normal results across completely included members instead of for a person. Obviously, individuals' singular gamble of sickness differs relying upon way of life and different variables. The benchmark hazard of cardiovascular sickness can be assessed utilizing a web-based number cruncher, for example, QRisk, which considers a scope of elements, for example, weight, smoking, pulse, cholesterol and age.
The probability of an individual creating cardiovascular illness in the following decade is communicated as a rate. For instance, consider an overweight 65-year-elderly person who smokes, has hypertension and absolute cholesterol. He might be at high gamble of cardiovascular sickness, contrasted and a 45-year-old, non-smoking lady with marginally raised cholesterol and pulse and no other gamble factors. Assuming a specialist were to survey their gamble of passing on in the following decade, the assessed risk for the man may be 38%, for instance, though the lady's gamble may be just 1.4%.
Presently consider the effect of taking statins for both. As indicated by the review, statins would lessen the general gamble of biting the dust by 9%. In outright terms, the man would decrease his gamble from 38% to 34.6%, and the lady from 1.4% to 1.3%.
Patients and their primary care physicians need to consider whether they think these gamble decreases are beneficial in a compromise between expected advantages and damages, including the bother of taking an everyday medication, potentially forever. This is especially notable for generally safe individuals for whom the advantages are peripheral. Nonetheless, individuals see risk diversely founded on their own insight and inclinations, and what could resemble a "great arrangement" to a might be viewed as of little worth to other people.
Our review features that patients and specialists should be upheld to settle on choices about medicines utilizing proof from every accessible review and introduced in an arrangement that assists them with getting likely advantages. The two patients and their primary care physicians need to comprehend the genuine effect of prescriptions to settle on informed choices. Depending on relative gamble, which is mathematically more great, rather than outright, may lead the two specialists and patients to misjudge the advantages of intercessions.
For instance, one investigation discovered that specialists evaluated a treatment as more viable and were bound to endorse it when the advantages were introduced as relative as opposed to as outright gamble decreases. Another overview viewed that most respondents would concur as evaluated for disease whenever gave relative gamble decreases, while simply over half would whenever gave outright gamble decreases.
In the event that you have been recommended statins, don't quit taking your drug without first counseling your PCP. Your gamble profile could imply that they could help you. In any case, on the off chance that you might want to reevaluate taking this medication, request that your PCP make sense of your outright gamble decrease and afterward settle on a cooperative choice.
Social Plugin